Last updated:
Disease groups:
Mpox is an infectious disease caused by the monkeypox virus (MPXV). It spreads through contact with infected people or animals, but you can take steps to protect yourself. We monitor and report on case numbers and trends and provide guidelines to minimise the risk.
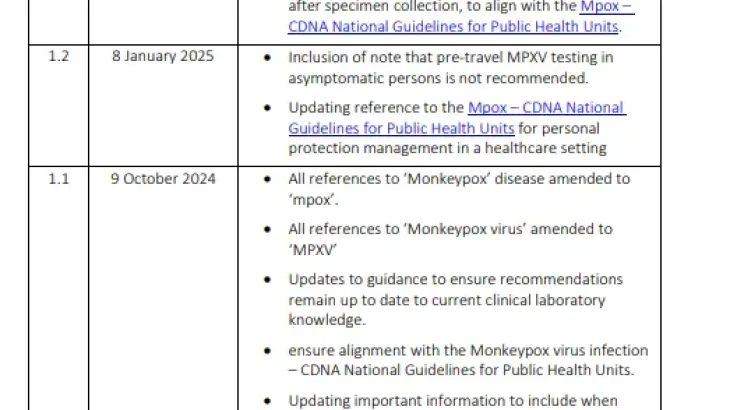
Mpox (formerly called monkeypox) is caused by infection with MPXV, which is related to the smallpox virus.
Most infections are mild, but in some cases, mpox can cause serious illness.
MPXV has evolved into different types of viruses, named clade I and clade II. Clade I is more likely to cause severe illness and death than clade II.
Mpox has been an important public health problem in some overseas countries for some time.
In 2022, mpox infections increased globally, and the virus spread to new countries that had not had mpox before.
In Australia:
Mpox can be serious, especially for people at greater risk of severe disease. Even for people with mild infections, mpox can be painful and recovery can take many weeks.
Anybody who is exposed to the virus can get mpox. Many cases in Australia have been among gay, bisexual and other men who have sex with men (GBMSM) or people who have sex with people who are GBMSM.
Reducing stigma around mpox is an important public health priority. People at increased risk of exposure need appropriate information and support.
Because of these impacts, we:
If you’re looking for advice about your own health or treatment options, see healthdirect or speak with a qualified healthcare professional. Our role is to provide public health advice – information and guidance that helps prevent disease, protect communities and improve wellbeing at a population level.
If you have severe symptoms or are worried, contact your nearest hospital immediately for urgent medical attention.
Common symptoms include:
Although some people with mpox don’t get a rash, you can get the mpox rash on any part of your body.
It can look like pimple-like lesions or sores and goes through several stages as the disease progresses.
The lesions can be very painful, especially in sensitive areas like the mouth or rectum.
Most people with mpox get better in 2 to 4 weeks.
Mpox can cause serious complications such as:
healthdirect’s symptom checker can help you work out whether you need to seek medical help.
Symptoms usually start between 3 and 21 days after getting infected.
Over time, the virus has evolved to spread more easily between people.
Mpox usually spreads during close contact with an infected person. This can include through:
Mpox can also spread:
We are still learning about all the ways mpox spreads between people and how often people without symptoms spread the virus to someone else. We monitor the latest evidence.
Mpox can be spread to others from up to 4 days before symptoms start.
People with mpox are considered infectious:
Mpox vaccines are available for people at greater risk of exposure or who have been exposed to mpox within the past 14 days. Read about mpox vaccinations available in your state or territory.
You should:
You should:
If you have had contact with a person with clade I mpox, there may be extra steps you need to take. Your state or territory health department or healthcare professional will advise you.
You should:
You should:
Follow the advice of your healthcare professional and state or territory health department if you:
Some people are at greater risk of being exposed to mpox or getting very sick from it.
Mpox can spread quickly in certain settings, including:
If you are at greater risk of severe disease, it is especially important to take steps to protect yourself.
Mpox poses a greater risk of severe illness for people who are:
Children aged under 10 years are more like to get:
People are more likely to be exposed to mpox if they:
When mpox is circulating in the community, people may be at greater risk of exposure if they are:
Read more information for GBMSM and find an mpox vaccination service.
Your healthcare professional can diagnose mpox with a test using swabs taken from affected areas.
They may recommend testing for sexually transmissible infections or other diseases that cause similar symptoms at the same time.
You can use healthdirect’s directory to find a health service near you.
Most people with mpox have mild symptoms that they can manage at home by staying hydrated and taking over-the-counter pain medication.
Some patients may need to go to hospital for treatment to manage their symptoms or complications.
Read more about how to manage or treat mpox.
Mpox is a nationally notifiable disease – these are diseases that present a risk to public health.
Health authorities in each state and territory report new confirmed and probable cases to us through the National Notifiable Diseases Surveillance System.
This is part of our surveillance activities, which help us monitor case numbers around the country and understand disease patterns.
We analyse the data and report on mpox case numbers through our data visualisation tool, where you can filter and search the latest information.
Public health units respond to mpox outbreaks in high-risk groups and settings. They might:
Settings may implement extra infection prevention and control actions to help reduce the spread of mpox. These include:
Read more about how the Australian Government defines and plans for outbreaks and pandemics.
For more information, see:
For information about mpox and vaccination in your state or territory see:
If you need mental health support, see a list of organisations, websites and services that offer support, counselling and information.
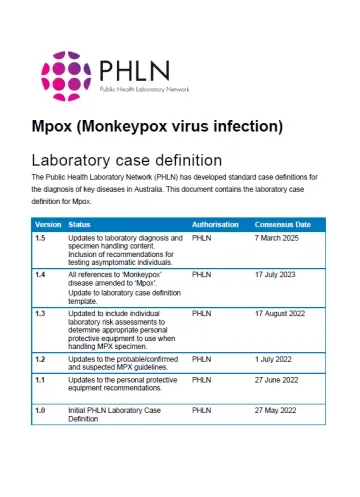
MPXV is an enveloped, double-stranded deoxyribonucleic acid virus of the genus Orthopoxvirus, which also includes variola virus (which causes smallpox).[1]
MPXV has 2 distinct genetic clades – I and II, each with 2 subclades – a and b.
The natural reservoir of MPXV is unknown. The virus has been isolated from several species of African rodents and primates.[2]
Read more about the different clades of MPXV.
Mpox is usually self-limiting with symptoms lasting 2 to 4 weeks.
The illness may start with prodromal symptoms including:
A maculopapular rash usually appears 1 to 5 days after the fever starts. It can be widespread or localised.
The rash progresses through several stages:
These sores eventually crust over and scab, usually within 14 to 21 days. They often leave behind scars.
The mpox rash can involve very few or no visible lesions, especially for clade IIb infections. When sexually acquired, lesions might only appear in the oral or anogenital regions.
Mpox can cause severe pain, especially if lesions are in sensitive areas like the mouth or rectum.
Complications of mpox can include:
Reinfections and infections in vaccinated people can occur, but the clinical presentation might be milder.
Read more about the clinical features of mpox.
Mpox can spread widely and cause severe illness, particularly in children and people who are immunocompromised.
The World Health Organization (WHO) has declared mpox a Public Health Emergency of International Concern twice since 2022. This is due to changes in disease epidemiology, including increasing case numbers and spread to new countries.
Over time, the virus that causes mpox has mutated to spread more easily between humans.
Surveillance and prevention activities, including vaccination and public health communications, help control outbreaks and protect priority populations.
Mpox primarily spreads through close contact, including sexual contact, and can spread quickly through sexual networks. Anyone who is exposed to mpox can be infected.
In Australia, a high proportion of cases have been among gay, bisexual and other men who have sex with men (GBMSM).
Reducing stigma around mpox infection is an important public health priority to ensure priority populations and people exposed to mpox:
Since 2022, a global outbreak of mpox clade IIb has resulted in more than 100,000 cases in 127 countries. Many cases in this outbreak have been in males, primarily GBMSM.
Since late 2023, an outbreak of clade Ib cases has been reported in the Democratic Republic of the Congo and neighbouring countries. Cases have been reported in several countries outside Africa, among people who travelled to epidemic regions.
Globally, infections with clade Ia have been associated with higher mortality rates than other subtypes.[3]
In Australia:
For the latest information on cases of mpox in Australia see the National Communicable Disease Surveillance data visualisation tool.
See more global mpox case data, including deaths.
Mpox mainly transmits directly through close or intimate contact with an infected person. This can be through broken skin or via mucous membranes in the:
This includes through sexual contact.[5]
It can also be spread through:
The incubation period ranges from 3 to 21 days.
A very small proportion of people might develop symptoms after 21 days from exposure.[6]
People can be infectious from 4 days before the onset of symptoms until both:
This normally takes 2 to 4 weeks.
People with no visible lesions are considered infectious until 21 days after the start of their symptoms, provided all symptoms have resolved.
Asymptomatic people are considered infectious for 21 days after a positive test.
Mpox poses a greater risk of severe illness for people who are:
Children aged less than 10 years are at higher risk of:
Pregnant people with mpox are at higher risk of miscarriage and stillbirth.[9]
Read more about mpox in:
People are more likely to be exposed to mpox if they:
When mpox is circulating in the community, people may be at greater risk of exposure if they are:
See what measures can prevent mpox infection.
Mpox can spread in settings where there is likely to be close, sustained physical contact between people.
These include:
Aboriginal and Torres Strait Islander communities might be at greater risk of spread due to:
Depending on the nature of cases and disease spread, public health units may take extra steps to reduce the risk to people in the community. Community actions must be co-designed and culturally appropriate.
Primary preventive vaccination is recommended for people at greater risk of exposure to mpox, including:
Primary preventive vaccination can also be considered for:
Post-exposure preventive vaccination may be offered to contacts of an mpox case to reduce their risk of becoming infected.
See the Australian Immunisation Handbook for more information about mpox vaccination and what is available in your state or territory.
When mpox is circulating in the community, prevention measures include:
People at greater risk of exposure should:
See more mpox resources.
Mpox is usually diagnosed through laboratory testing using nucleic acid amplification testing.
The type of specimen collected depends on whether lesions are present and their stage. Specimens include:
A full screen for HIV and sexually transmissible infections is often done at the same time.
Read more about mpox:
Mpox is usually a self-limiting disease with symptoms lasting 2 to 4 weeks. Most people don’t need specific treatment. Some patients require supportive therapy, such as medications to manage their pain.
People with severe mpox or complications, or those at high risk of severe disease, may be prescribed an antiviral medication.
Read more about:
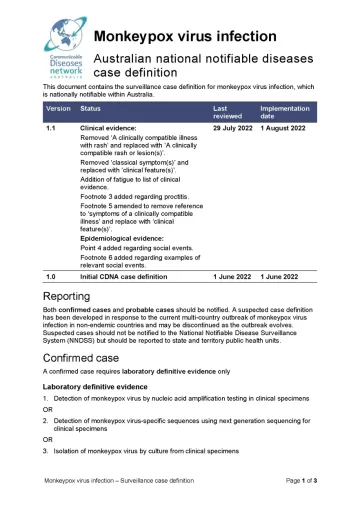
Confirmed and probable mpox cases are nationally notifiable in Australia. This means certain health professionals must report diagnoses through their relevant health authorities.
Check how to report confirmed and probable mpox cases in your state or territory:
State and territory health authorities report new cases to us daily through the National Notifiable Diseases Surveillance System.
We report case numbers through our data visualisation tool, where you can filter and search the latest information, as part of our surveillance activities.
This helps us to:

Public health units urgently investigate all confirmed, probable and suspected mpox cases. The public health management of cases focuses on:
Public health units generally advise people with mpox to:
To help prevent spread of mpox within households, people with mpox should:
Public health units may recommend extra precautions, such as isolation, where there is a reasonable suspicion of infection with MPXV clade I.
The public health unit or treating clinician will advise the person when they have been cleared to resume normal activities.
For 12 weeks after clearance, people who have had mpox should:
Public health units undertake contact tracing to:
Post-exposure prophylaxis (PEP) may be offered to contacts of an mpox case to reduce their risk of becoming infected. This may involve vaccination or antiviral medication.
Read more about PEP with vaccination and antiviral medications.
Other contact management actions may include:
Exclusions and restrictions may apply for workers in some high-risk settings.
Public health units may recommend extra precautions, such as advice to work from home, where there is a reasonable suspicion of contact with a case infected with MPXV clade I.
The way public health units respond to mpox outbreaks depends on the setting and nature of the outbreak.
In some special situations and high-risk settings, specific control measures, including post-exposure preventive vaccination, may be implemented to manage outbreaks.
Enhanced infection prevention and control measures may also reduce the risk of transmission. This may include:
Extra public health actions may be implemented in some special situations and high-risk settings when mpox is circulating in the community or a case is identified. These include:
Prevention and control measures in these settings can include:
See the:
For information about mpox and vaccination in your state or territory see: