Last updated:
Disease groups:
Influenza (flu) is a common viral infection of the respiratory tract. It most often spreads through respiratory droplets. The best way to protect yourself is to get vaccinated. The best way to protect others is to stay at home when you are sick.
Flu is a common and highly contagious respiratory infection.
Most infections are caused by influenza A or B viruses, but there are many subtypes and strains.
Flu can cause mild to severe illness. Most people recover within a few days, but some people are at greater risk of getting severely unwell.
The number of people with flu usually peaks in winter but people can get infected at any time of year, especially in tropical regions.
Each year in Australia, flu causes about:
Flu viruses change (mutate) easily.
Small, gradual changes to flu viruses (called antigenic drift) cause seasonal outbreaks. That’s why the flu vaccine is updated each to year to better match the strains most likely to be circulating.
Because flu viruses change over time, it’s hard to predict how severe the flu season will be each year. Some seasons are worse than other depending on:
Large sudden changes (called antigenic shift) can create new subtypes and strains. If people have little immunity to a new strain, a serious outbreak – or rarely, a pandemic – is possible.
If you’re looking for advice about your own health or treatment options, see healthdirect or speak with a qualified healthcare professional. Our role is to provide public health advice – information and guidance that helps prevent disease, protect communities and improve wellbeing at a population level.
Common symptoms include:
Symptoms can range from mild to severe, and not everyone experiences every symptom.
Symptoms usually improve within a few days to a week, but a cough can last longer.
Complications can include:
healthdirect’s symptom checker can help you decide whether to see a health professional.
Symptoms usually start about 2 days after getting infected, but this can range from 1 to 4 days.
Flu mainly spreads through droplets from an infected person’s respiratory tract. When people talk, cough or sneeze, these droplets travel through the air and land on people and surfaces.
Other people can get infected when droplets:
Read more about how flu spreads.
People with flu are usually most infectious in the first 3 days after symptoms appear.
But the virus can usually be spread from 1 day before symptoms start until about 7 days after, and sometimes longer (up to 10 days in children).
The best way to protect against flu is to get vaccinated each year, in April or May.
Flu vaccines are available to protect against the most common strains. In 2026, an intra-nasal vaccine is available for some children. Eligible people can get vaccines for free under the National Immunisation Program or state or territory programs. If you are not eligible for a free vaccine, you can buy one from your health professional or pharmacy.
You can help protect yourself and others by:
Read more ways to prevent the spread of flu and other respiratory viruses.
Some people are at greater risk of getting flu or getting very sick from it.
It can spread quickly in homes and other settings including:
If you are at greater risk of severe disease, it is especially important to take steps to protect yourself. You should:
People at greater risk of severe illness include:
Anybody can be exposed to flu. But people who have a lot of close contact with others might be more likely to be exposed. This includes through their jobs, living situation, or recreational activities.
Flu is usually diagnosed through laboratory testing of a sample collected with a swab from the nose or throat.
Rapid antigen tests that can be done at home are also widely available from supermarkets and pharmacies.
Read more about how flu is diagnosed.
You can use healthdirect’s directory to find a health service near you.
Most people will get better without any treatment within 7 to 10 days. Healthcare professionals might prescribe antiviral medicines to people at risk of severe illness.
Antibiotics are not used to treat flu, because they do not work for viral infections. Taking antibiotics when you don’t need them can increase the risk of antibiotic resistance.
Read more about how to manage or treat flu.
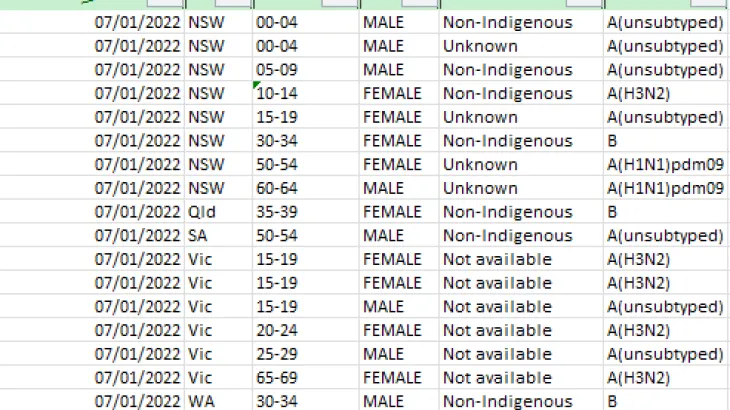
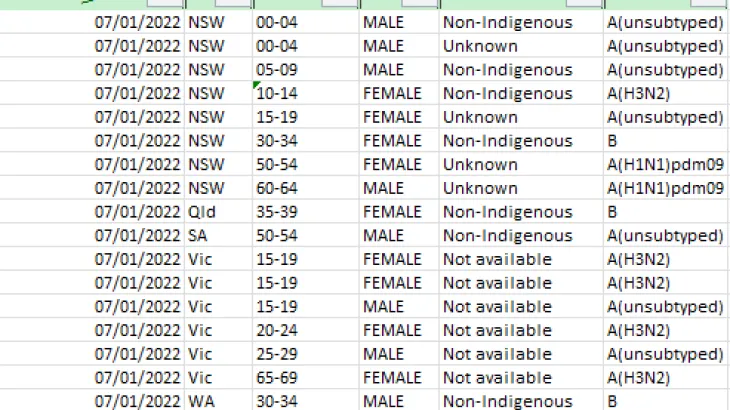
Influenza is a nationally notifiable disease – these are diseases that present a risk to public health.
Health authorities in each state and territory report new cases to us through the National Notifiable Diseases Surveillance System.
Flu data is also collected through other surveillance systems, guided by the Australian National Surveillance Plan for COVID-19, Influenza, and RSV.
We analyse the data, and report on flu case numbers through:
These are part of national surveillance to monitor case numbers and disease patterns.
Flu outbreaks are common, especially in winter months.
State and territory health departments provide guidance and support for outbreaks in some situations – for example, in residential aged care homes or hospitals.
In certain situations, such as when a new flu virus emerges, it can present a serious threat to Australia.
In these situations, we follow our action plans to limit the impact on the health of Australians and on our health system.
Read more about how the Australian Government defines and plans for outbreaks and pandemics.
For information about flu in your state or territory, see: